Pelvic Floor Dysfunction in Men: Symptoms, Causes, and Treatment
Pelvic floor dysfunction causes pain, urinary issues, and sexual problems in men. Most cases go undiagnosed for years. Symptoms, causes, and treatment options.
Pelvic floor dysfunction (PFD) in men is underdiagnosed — partly because most physicians receive limited training in male pelvic health, and partly because the symptom profile overlaps with several more commonly recognized conditions (prostatitis, overactive bladder, erectile dysfunction). Men with PFD frequently cycle through urological and gastroenterological workups for years before receiving an accurate assessment.
What the pelvic floor does
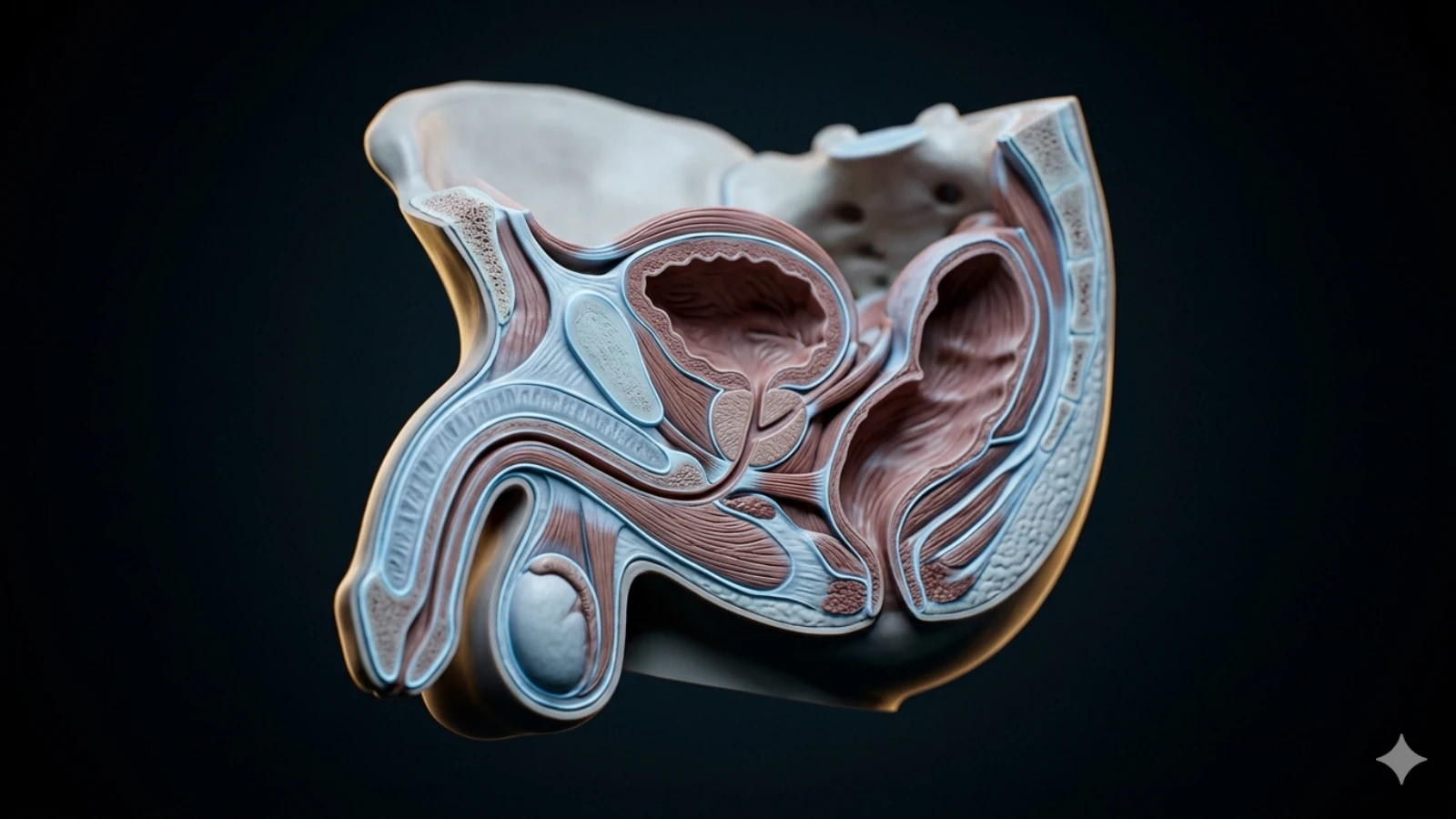
The male pelvic floor is a multilayered group of muscles, connective tissue, and fascia spanning the base of the pelvis. These structures:
- Support the bladder, bowel, and prostate
- Control urinary and bowel continence
- Coordinate with the external urethral sphincter during voiding
- Contribute to erectile function and ejaculation mechanics
- Stabilize the pelvis during movement
Unlike the more commonly discussed skeletal muscles, pelvic floor muscles function semi-automatically — mostly outside conscious awareness — which makes dysfunction harder to detect without targeted assessment.
The two types of dysfunction
Pelvic floor dysfunction is not a single condition. The two primary presentations have opposite mechanisms and opposite treatments.
Hypertonic dysfunction (overactive/tight pelvic floor): The muscles are chronically contracted and fail to relax properly. This is the more common presentation in men presenting with pelvic pain, and the most commonly misdiagnosed. A tight pelvic floor produces symptoms that paradoxically worsen with Kegel exercises — a critical diagnostic clue.
Hypotonic dysfunction (weak/underactive pelvic floor): The muscles lack adequate strength and endurance. This presents primarily as stress urinary incontinence (leakage with coughing, sneezing, exercise) and is common after prostatectomy. This is the presentation that benefits directly from Kegel training.
Symptoms by system
Urinary symptoms
- Urgency (sudden, compelling urge to urinate)
- Frequency (urinating more than 8 times per day, or waking multiple times at night)
- Incomplete emptying sensation
- Hesitancy or slow stream (in absence of structural BPH)
- Post-void dribbling
- Stress incontinence (leakage with exertion)
Bowel symptoms
- Constipation or difficulty with defecation
- Straining producing incomplete evacuation
- Rectal pain or pressure
- Painful defecation
Pain symptoms
- Perineal pain or pressure (between scrotum and anus)
- Scrotal or testicular aching (without pathological testicular cause)
- Rectal or tailbone pain
- Lower abdominal or suprapubic pain
- Pain that worsens with sitting and improves with walking
Sexual symptoms
- Erectile dysfunction (specifically difficulty maintaining erection)
- Pain with ejaculation
- Reduced ejaculatory force
- Post-ejaculatory aching or burning
- Pelvic heaviness or discomfort after sexual activity
Common causes and contributing factors
Chronic stress and tension holding: The pelvic floor responds to psychological stress the same way the jaw and shoulders do — with unconscious bracing. Men who habitually hold tension in their lower body frequently develop hypertonic PFD without any identifiable anatomical trigger.
Postural and occupational factors: Prolonged sitting (particularly with forward pelvic tilt), heavy weightlifting with poor bracing mechanics, and sedentary work combine to produce chronic pelvic floor loading.
Prior trauma: Perineal trauma (cycling injuries, falls), pelvic surgery, or prior prostatitis can initiate a protective muscle-guarding response that persists long after the original injury heals.
Prostatitis misdiagnosis: Clemens et al. (2019) [^clemens2019] found that a significant proportion of men diagnosed with chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) — the most common prostate diagnosis in men under 50 — have pelvic floor hypertonicity as the primary or contributing cause. This diagnosis should prompt pelvic floor assessment.
Post-prostatectomy: Prostatectomy disrupts the anatomical continuity of pelvic floor structures. Hypotonic dysfunction with stress incontinence is nearly universal immediately post-surgery; recovery varies significantly based on surgical approach, baseline pelvic floor health, and rehabilitation.
Diagnosis
Accurate diagnosis requires physical assessment by a pelvic floor physical therapist or urologist with pelvic floor training. Standard urological workup (urinalysis, PSA, cystoscopy) does not assess pelvic floor muscle function.
Assessment typically includes:
- External palpation of the perineum and pelvic attachment points
- Internal rectal examination to assess muscle tone, tenderness, and trigger points
- Assessment of resting tone, squeeze strength, coordination, and relaxation
- Evaluation of breathing pattern and intra-abdominal pressure management
Self-assessment is limited. The inability to consciously relax the pelvic floor on command (bear-down without straining) suggests hypertonicity. Leakage with coughing suggests hypotonic dysfunction.
Treatment approaches
Pelvic floor physical therapy
Physical therapy is the first-line treatment for both hypertonic and hypotonic PFD, with approaches specific to each presentation.
For hypertonic dysfunction, therapy focuses on:
- Manual release of trigger points (internal and external)
- Paradoxical relaxation training — learning to consciously release the pelvic floor
- Diaphragmatic breathing coordination (breath and pelvic floor movement are directly linked)
- Postural correction and movement pattern normalization
- Gradual exposure to positions and activities that provoke symptoms
Anderson et al. (2005) [^anderson2005] demonstrated that trigger point release combined with paradoxical relaxation training produced significant pain reduction in men with CP/CPPS — a population with a large proportion of pelvic floor hypertonicity.
For hypotonic dysfunction, therapy focuses on Kegel strengthening with biofeedback to ensure correct muscle activation (many men activate accessory muscles rather than the pelvic floor). Gevirtz (2010) [^gevirtz2010] reviewed biofeedback-assisted pelvic floor training for urinary control outcomes.
What to avoid
Men with hypertonic PFD should not perform Kegel exercises until hypertonicity has been resolved. Strengthening an already-tight muscle system increases symptoms. This is one of the most common errors in self-managed pelvic floor rehabilitation.
Heavy weightlifting with Valsalva breath-holding significantly increases intra-abdominal and pelvic floor pressure. Men with active PFD should limit or temporarily suspend heavy compound lifts (squats, deadlifts) and focus on pressure management before returning to loaded training.
Pain management adjuncts
For men with significant pelvic pain:
- Sitz baths (warm water perineal soaks) reduce muscle tension and improve circulation
- Avoiding prolonged sitting — standing desks, breaks every 30–45 minutes
- Trigger point self-massage via perineal pressure (a tennis ball or purpose-made tool)
- Avoiding constipation through dietary fiber and hydration (straining worsens pelvic floor tension)
When to seek care
Seek evaluation when pelvic symptoms persist beyond 3 months, interfere with work or relationships, or when initial conservative measures (rest, anti-inflammatory measures) produce no improvement. The chronic nature of untreated PFD — and its tendency to worsen under continued physical and psychological stress — makes early intervention significantly more effective than later.
Any acute onset of urinary retention, severe pelvic pain, fever with urinary symptoms, or blood in urine warrants immediate medical evaluation to rule out infection, obstruction, or other pathology.
References
- Cohen D, Gonzalez J, Goldstein I. Pelvic floor physical therapy for male pelvic pain. Current Sexual Health Reports (2016). PubMed:28018185
- Anderson RU, Wise D, Sawyer T, Chan CA. Trigger point release and paradoxical relaxation training in men with chronic pelvic pain syndrome. Journal of Urology (2005). PubMed:15758765
- Gevirtz R. Pelvic floor biofeedback in patients with urinary incontinence: a randomized controlled trial. Biofeedback (2010). PubMed:27182497
- Clemens JQ, Meenan RT, O'Keeffe Rosetti MC, Gao SY, Calhoun EA. Prevalence of and risk factors for prostatitis: population based assessment using physician assigned diagnoses. Journal of Urology (2019). PubMed:16469861
Pelvic Floor Function Self-Assessment
Anonymous · 5 minutes · No account needed
Related Articles
 Tier 1 · Pelvic Floor
Tier 1 · Pelvic FloorPelvic Floor Relaxation for Men: Releasing Hypertonic Tension
A tight pelvic floor causes pain and dysfunction — the opposite problem from weakness. Relaxation techniques, breathing, and trigger point release explained.
 Tier 1 · Pelvic Floor
Tier 1 · Pelvic FloorPelvic Floor Exercises for Erectile Dysfunction: What the Evidence Shows
Pelvic floor training improves erectile function in 40-75% of men. Stronger evidence than pills for some populations. Protocol and mechanisms explained.
 Tier 1 · Pelvic Floor
Tier 1 · Pelvic FloorThe Male Pelvic Floor: A Muscle Group Most Men Have Never Deliberately Used
The pelvic floor controls far more than urinary continence. Here's what it actually does, why it weakens, and how to train it — with evidence.