The Male Pelvic Floor: A Muscle Group Most Men Have Never Deliberately Used
The pelvic floor controls far more than urinary continence. Here's what it actually does, why it weakens, and how to train it — with evidence.
Ask a man to contract his pelvic floor and you'll get one of two responses: a blank stare, or an approximation of something he half-remembers from a pamphlet in a urology waiting room.
This is a problem, because the pelvic floor is doing a significant amount of work for him regardless of whether he knows it's there. It's involved in urinary control, ejaculation timing, erectile rigidity, bowel function, and lumbar spine stabilization. Most men interact with it only when something goes wrong.
This piece is about how it works, what goes wrong, and how to deliberately train it.
What the pelvic floor actually is
The pelvic floor is a hammock-shaped group of muscles and fascia spanning the base of the pelvis from the pubic bone anteriorly to the coccyx posteriorly. In men, it has three primary functional layers:
Superficial layer — bulbospongiosus and ischiocavernosus muscles. These wrap around the base of the penis and are directly involved in ejaculation (bulbospongiosus rhythmic contractions) and in compressing the crura to assist erection rigidity.
Deep layer — levator ani complex, including the pubococcygeus, iliococcygeus, and puborectalis. This is the primary load-bearing structure. It supports the bladder, prostate, and rectum, and its tone directly affects urinary continence.
Urethral and anal sphincters — technically separate but functionally integrated with the pelvic floor. Voluntary control of both depends on a healthy, coordinated pelvic floor.
Lavoisier et al. (1988) [^lavoisier1988] documented the reflex coordination between voluntary pelvic floor contractions and penile rigidity, establishing the neurophysiological link that makes pelvic floor training relevant to erectile function — not just incontinence.
Why it weakens
Unlike peripheral skeletal muscles, the pelvic floor is a postural muscle: it's meant to maintain tone continuously, not just during discrete contractions. It weakens for several specific reasons:
Prolonged sitting — hours of posterior pelvic tilt flatten the natural curvature of the spine and put the pelvic floor in a chronically lengthened position. Sustained lengthening without adequate load leads to decreased resting tone over time.
Prostate procedures — radical prostatectomy and TURP (transurethral resection of the prostate) directly disturb the anatomical structures supporting the pelvic floor. Stafford et al. (2016) [^stafford2016] found that structured pelvic floor training before and after prostatectomy significantly improved continence recovery rates at 12 months.
Aging — Type I (slow-twitch) muscle fiber density declines with age in the pelvic floor as elsewhere. Siegel et al. (2014) [^siegel2014] identified pelvic floor dysfunction as a significant contributing factor to lower urinary tract symptoms (LUTS) — urgency, frequency, incomplete emptying — that are often attributed entirely to prostate enlargement.
High-impact sports without concurrent pelvic floor training — distance running, heavy lifting, and sports involving repetitive ground-impact create significant intra-abdominal pressure. Without adequate pelvic floor bracing capacity, these loads are poorly managed and can contribute to stress urinary incontinence or pelvic organ prolapse over time.
The evidence for training
The landmark RCT is Dorey et al. (2004) [^dorey2004], which compared structured pelvic floor muscle training against sham exercises in men with erectile dysfunction of at least six months' duration. At three months, 40% of the intervention group had regained normal erectile function, compared to 5% of the sham group. The effect was maintained at six months in the majority of responders.
The mechanism is not mysterious: ischiocavernosus and bulbospongiosus contractions contribute to the rigidity phase of erection by compressing the deep dorsal vein of the penis, reducing venous outflow and maintaining intracavernous pressure. Weak or poorly coordinated pelvic floor muscles cannot sustain this compression effectively.
For ejaculatory control, Manley et al. (2018) [^manley2018] reviewed the evidence for pelvic floor training in premature ejaculation. The systematic review found meaningful improvement in intravaginal ejaculatory latency time (IELT) across studies, though methodological heterogeneity limits firm conclusions. The proposed mechanism: voluntary pelvic floor contraction can interrupt the ejaculatory reflex if learned with sufficient proprioceptive awareness.
How to actually train it
The clinical protocol for pelvic floor rehabilitation involves three elements: isolation, endurance, and integration.
Step 1: Isolation (finding the right muscles)
The most reliable cue for locating the correct muscle group: imagine you are stopping the flow of urine midstream and simultaneously preventing passing gas. The contraction should feel internal and upward — not a tensing of the glutes, abdomen, or thighs.
Common errors:
- Holding the breath (indicates straining, not pelvic floor isolation)
- Buttock clenching (activates gluteus maximus, not levator ani)
- Abdominal bracing (involves the wrong muscle group entirely)
If you're unsure whether you're contracting the right muscles, a physiotherapist specializing in pelvic health can provide biofeedback-guided assessment. This is not an unusual request — it's the standard clinical approach.
Step 2: Endurance component (slow-twitch fiber training)
Protocol:
- Contract and lift: hold for 5–10 seconds
- Fully release: allow complete relaxation before the next repetition
- 8–12 repetitions per set
- 3 sets daily
The release phase matters as much as the contraction. Chronically hypertonic pelvic floors — where the muscles are in a state of excessive tension rather than healthy tone — cause their own set of problems (pelvic pain, voiding dysfunction, painful ejaculation). Training toward full, deliberate relaxation between contractions prevents this.
Progress marker: work toward 10-second sustained holds with complete relaxation.
Step 3: Power component (fast-twitch fiber training)
Protocol:
- Quick, maximal contraction: 1–2 seconds
- Full release
- 10–15 repetitions
- 1–2 sets daily
This trains the reflex bracing capacity needed for coughing, sneezing, and heavy lifting — events that produce sudden intra-abdominal pressure spikes.
Integration into movement
The goal is not isolated pelvic floor contractions in a gym setting — it's a pelvic floor that functions correctly during real activities. Clinical progression:
- Weeks 1–4: supine (lying on back), isolated contractions
- Weeks 5–8: seated and standing contractions
- Weeks 9–12: integrated with lifting, walking, exercise
A pelvic floor that contracts correctly during a heavy deadlift or during intercourse requires this functional integration — not just the ability to hold a contraction for 10 seconds while lying still.
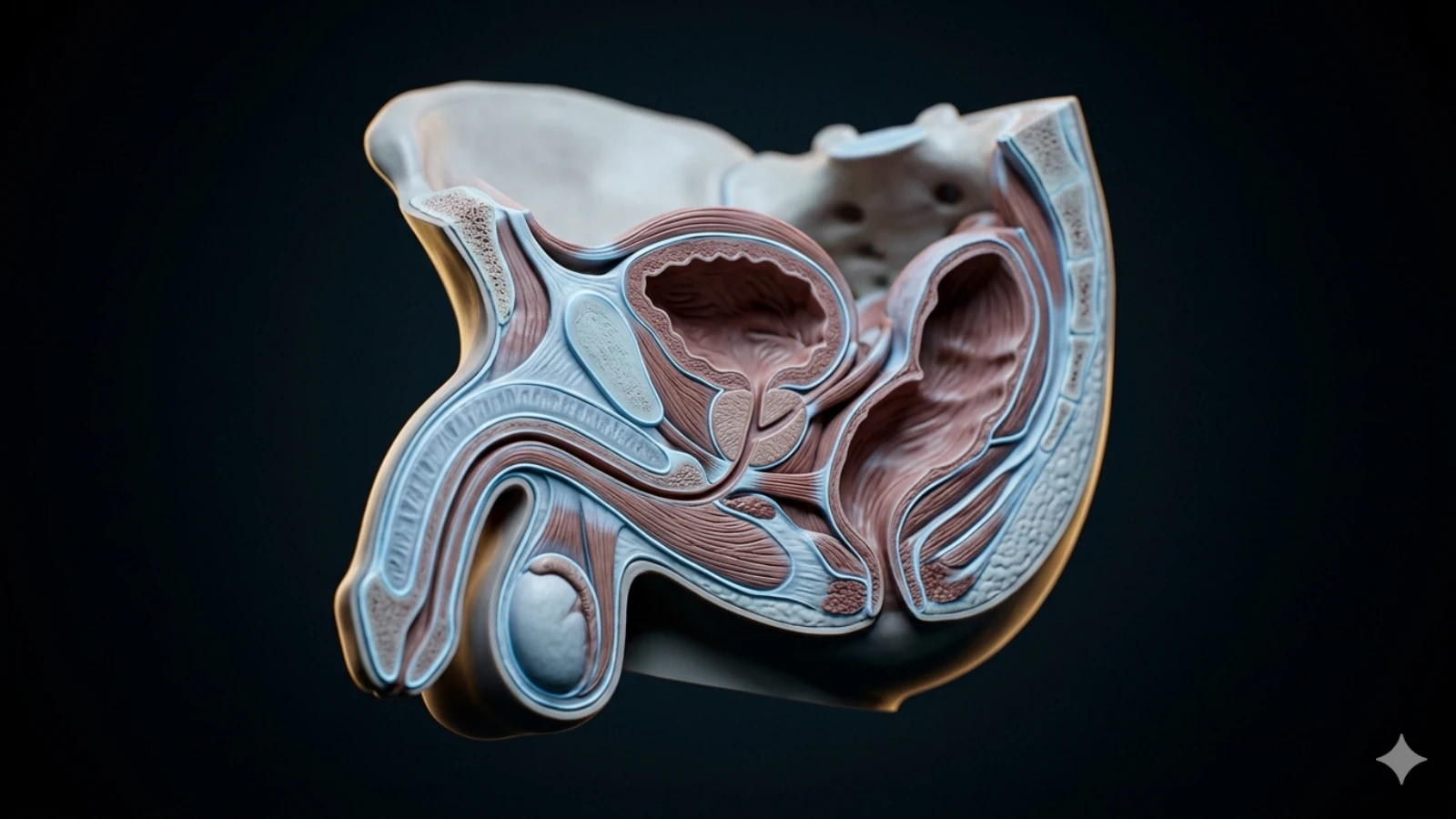
The prostate connection
The prostate sits directly superior to the pelvic floor, resting on the levator ani. Prostate massage — whether for prostatitis symptom management or otherwise — is more effective and more comfortable when the surrounding pelvic floor musculature is neither hypertonic (too tight) nor atrophic (weakened). This is the anatomical reason pelvic floor training is a foundation before more advanced prostate health work.
If you have never deliberately engaged your pelvic floor, the assessment quiz below is a reasonable starting point for understanding your prostate health context.
References
- Stafford RE, Ashton-Miller JA, Constantinou C, Coughlin G, Lutton N, Hodges PW. Pelvic floor muscle training for erectile dysfunction and climacturia 1 year after radical prostatectomy. The Prostate (2016). PubMed:26773612
- Dorey G, Speakman MJ, Feneley RC, Swinkels A, Dunn CD. A randomised controlled trial of pelvic floor muscle exercises to treat erectile dysfunction. BJU International (2004). PubMed:15529991
- Lavoisier P, Proulx J, Courtois F. Perineal contraction: a reflex response to voluntary pelvic floor muscle contraction. Journal of Urology (1988). PubMed:3357357
- Siegel SW et al.. The importance of pelvic floor muscle dysfunction in the cause and treatment of lower urinary tract symptoms. Journal of Urology (2014). DOI:10.1016/j.juro.2013.10.082
- Manley C, Bour M, Roper J. Pelvic floor muscle training for premature ejaculation: a systematic review. International Journal of Impotence Research (2018). DOI:10.1038/s41443-018-0053-1
Pelvic Floor Function Self-Assessment
Anonymous · 5 minutes · No account needed
Related Articles
 Tier 1 · Pelvic Floor
Tier 1 · Pelvic FloorPelvic Floor Exercises for Erectile Dysfunction: What the Evidence Shows
Pelvic floor training improves erectile function in 40-75% of men. Stronger evidence than pills for some populations. Protocol and mechanisms explained.
 Tier 1 · Pelvic Floor
Tier 1 · Pelvic FloorPelvic Floor Dysfunction in Men: Symptoms, Causes, and Treatment
Pelvic floor dysfunction causes pain, urinary issues, and sexual problems in men. Most cases go undiagnosed for years. Symptoms, causes, and treatment options.
 Tier 1 · Pelvic Floor
Tier 1 · Pelvic FloorPelvic Floor Relaxation for Men: Releasing Hypertonic Tension
A tight pelvic floor causes pain and dysfunction — the opposite problem from weakness. Relaxation techniques, breathing, and trigger point release explained.