Prostate Massage: Technique, Anatomy, and What to Expect
Practical technique for prostate massage — location, correct approach, sensation progression, and device use. For therapeutic and pleasure purposes.
The previous articles in this series established the anatomy (the prostate's innervation, location, and role in sexual function) and the clinical evidence for prostate massage in prostatitis management. This article addresses the practical technique — what you actually do, in what sequence, and what to expect at each stage.
This is written for two overlapping audiences: men approaching prostate stimulation primarily from a therapeutic/health maintenance perspective, and men approaching it primarily from a pleasure perspective. The anatomy is the same. The technique principles are largely the same. The difference is in pacing and intent.
Prerequisites
Arousal state matters more than most guides acknowledge. During sexual arousal, the prostate engorges with blood — increasing its size, prominence, and sensitivity. Attempting prostate stimulation in an unaroused state is the most common reason first attempts fail. The prostate at baseline may be difficult to locate clearly; the aroused prostate is firmer, more prominent, and more responsive to pressure.
The practical recommendation: approach this during, or after significant time spent in, a state of sexual arousal — not as a clinical procedure to perform on an unaroused body.
Bowel timing. For rectal insertion (whether finger or device), comfort is highest 2–4 hours after a bowel movement, when the rectum is naturally empty. You do not need to do anything elaborate — this is the natural physiological state for most people during those hours.
Cleanliness. External cleaning with mild soap and water is sufficient for any rectal exploration. If you prefer an enema, warm water only — commercial enema solutions can irritate the rectal mucosa and increase discomfort.
Anatomy in practice
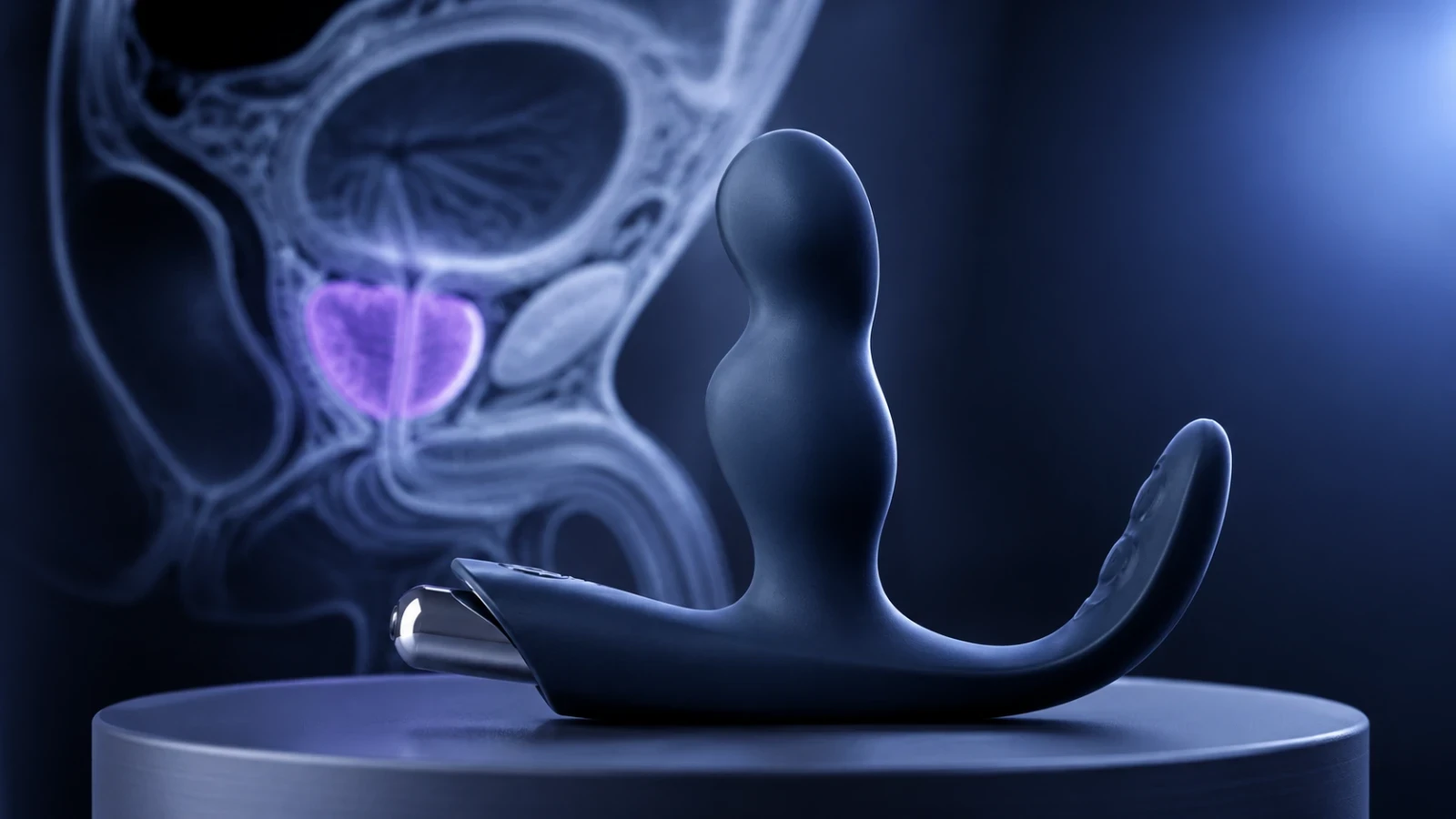
The prostate is located on the anterior (front) wall of the rectum — the wall facing toward your navel when you are lying on your back. Its position is typically described as 5–8 cm from the anal verge, but the practical landmark is texture and response, not distance.
What does the prostate feel like? It has a distinct texture from the surrounding rectal tissue — firmer, with a central furrow (the median sulcus) that separates the two lateral lobes. In an unaroused man it may feel like a smooth firm region slightly different in consistency from the softer surrounding tissue. In an aroused man it becomes more prominent and distinct, and applying pressure to it typically produces an unmistakable sensation — a combination of deep pressure and a sensation that's often described as "needing to urinate" at first, which is a normal misinterpretation of pelvic afferent activation.
Levin (2018) [^levin2018] documented the mechanoreceptors in the prostatic capsule — pressure against the gland activates these directly, which is why the sensation is immediate and distinct rather than diffuse.
Digital technique
Position: The most accessible starting position is lying on your back with your knees drawn toward your chest, or on your side with the same. This opens the rectum and reduces the angle needed for anterior access. Sitting on the toilet or squatting also works — gravity helps in these positions.
Lubrication: Use significantly more lubricant than you think necessary. Water-based lubricant only (not silicone-based, which is incompatible with silicone devices). Apply to the external area first, then to the inserting finger. Reapplication during is normal.
Insertion: Insert slowly, with constant gentle pressure rather than in and out movements initially. The external sphincter has a natural "guarding" reflex — allowing it to relax (rather than forcing past it) takes a moment but produces dramatically more comfort. Once past the first sphincter (external), there is a natural sense of relaxation — continue inward.
Locating the prostate: Once inserted to roughly 5–7 cm, curve the finger anteriorly (toward your navel). You are feeling for the firmer zone on the anterior wall. If you're not sure you've found it, this is expected in the first attempt — the aroused state makes it significantly more distinct.
Technique once located: The most effective approach is firm sustained pressure against the gland, with gentle rhythmic pressure variations, rather than vigorous in-and-out movement. The sensation builds over several minutes of consistent contact — this is the visceral afferent threshold effect described in the neuroscience article. Expecting an immediate intense response produces disappointment; allowing for the cumulative buildup produces the characteristic response.
The perineum: Simultaneously applying external pressure to the perineum — the area between the scrotum and anus, which corresponds to the external surface of the pelvic floor musculature directly beneath the prostate — creates dual afferent input. This is why prostate devices include a perineal tab; you can replicate this manually during digital exploration.
Device technique
The principles above apply to devices — the difference is that a correctly curved device (see the device buying guide) maintains consistent position and pressure without requiring sustained muscular effort, which is what makes the "hands-free" approach that most prostate devices are designed for both practical and effective.
Insertion of Helix Syn: Apply generous water-based lubricant. Insert with the narrow tip first, curved toward the anterior wall. The perineal tab should rest externally in the perineal groove. Once positioned, the device should remain in place without manual holding.
What happens next: Most men using a prostate device for the first time experience the sensation of "something is there" but no immediate dramatic response. This is correct — you are in the right position. The response builds with:
- Continued arousal (maintaining or building sexual arousal)
- Pelvic floor contractions: voluntary contractions of the pelvic floor muscles cause the device to move slightly and rhythmically stimulate the gland. Light rhythmic contractions (not maximal clenching) produce more stimulation than rigid holding.
- Time: 20–40 minutes of patient, engaged stimulation is typical for first experiences to produce characteristic effects
What to expect: the typical progression
First attempts: Likely awareness of the location and a novel sensation. Possibly some of the "needing to urinate" misinterpretation. Some men reach full response; most need multiple sessions to learn the pathway.
With experience: The characteristic prostatic sensation — a deep diffuse warmth or pressure that builds and integrates with genital arousal — becomes more accessible and faster to reach as the nervous system learns the pathway. This is neurological habituation in reverse: learning the pathway makes it more readily activatable.
Combined stimulation: The most consistently reported intense experience combines prostate stimulation with penile stimulation. The two afferent pathways — somatic genital and visceral prostatic — converge at the spinal cord and produce combined activation that most men report as more intense than either alone.
Clinical context note
If your interest in prostate massage is primarily therapeutic (management of chronic prostatitis, Category II or IIIa), the technique principles above apply, with emphasis on methodical expressed prostatic secretion rather than pleasure optimization. Nickel et al. (1999) [^nickel1999] used twice-weekly sessions in their clinical protocol — consistency matters more than intensity for therapeutic benefit. The clinical and the sensory are not mutually exclusive: therapeutic benefit and pleasurable response can coexist in the same session.
Related reading
- Prostate massage devices: buying guide — device selection for sustained pressure at the correct anatomical position
- First prostate orgasm: what to expect — what the first sessions typically produce and the realistic learning curve
- Prostate orgasm: anatomy and neuroscience — the neurological basis for the technique described here
- Prostate massage: clinical evidence and medical use — evidence base for therapeutic applications of the same technique
References
- Levin RJ. The prostate gland and its role in the physiology of male sexual arousal. Clinical Anatomy (2018). DOI:10.1002/ca.22990
- Nickel JC, Downey J, Young I, Boag S. Repetitive prostatic massage therapy for chronic refractory prostatitis. Techniques in Urology (1999). PubMed:10527258
Related Articles
 Tier 3 · Sexual Wellness
Tier 3 · Sexual WellnessProstate Massage Devices: A Science-Informed Buying Guide
Device selection for prostate stimulation mapped to anatomy. What device characteristics actually matter, what to look for, and how to choose.
 Tier 3 · Sexual Wellness
Tier 3 · Sexual WellnessP-Spot vs G-Spot: A Neural Pathway Comparison
The P-spot and G-spot share homologous anatomy and analogous neural pathways. Here is the neuroscience explaining why they produce similar reported experiences.
 Tier 3 · Sexual Wellness
Tier 3 · Sexual WellnessThe P-Spot: Precise Anatomy, Distinct Sensation, and Neurophysiological Basis
The prostate, or P-spot, offers unique sexual sensations distinct from penile stimulation due to its rich, specific innervation and deep visceral pathways.